
The air you breathe is invisible. So is the damage it can cause — until it isn’t.
Most people think of air pollution as an outdoor problem: smoggy skylines, traffic fumes, industrial smokestacks. But the impact of polluted air is deeply, physically personal. It plays out inside your bronchial tubes, in the walls of your alveoli, in the inflammatory responses your immune system launches every time you inhale a lungful of particle-laden air. It happens continuously, invisibly, and cumulatively — and by the time most people notice symptoms, years of subclinical damage have often already occurred.
This guide explains what air pollution actually does to lung tissue, who faces the greatest risk, what the warning signs look like, and — crucially — what evidence-based steps can meaningfully protect your respiratory health.
What Air Pollution Actually Contains
“Air pollution” is a catch-all term that encompasses a diverse mix of physical particles, chemical gases, and biological contaminants. Not all of them affect the lungs in the same way.
Particulate Matter: The Most Dangerous Component
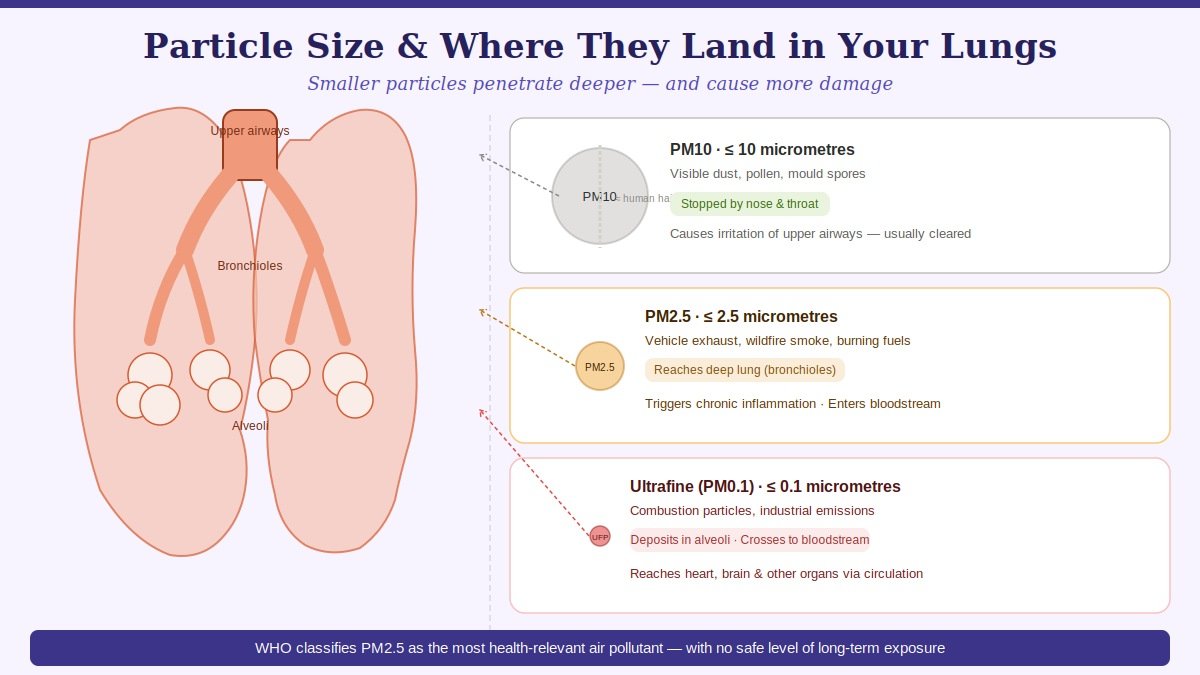
Particulate matter (PM) is classified by size — and size determines where particles deposit in the respiratory tract and how much damage they cause.
PM10 (particles ≤10 micrometres in diameter) are filtered relatively effectively by the nose and upper airways. They cause irritation and inflammation in the upper respiratory tract but rarely penetrate to the deep lung.
PM2.5 (particles ≤2.5 micrometres) are the most clinically significant fraction. Too small to be filtered by nasal hairs or the mucociliary escalator of the upper airways, they travel directly into the bronchioles and alveoli — the deepest, most delicate regions of the lung. From the alveolar surface, ultrafine particles can cross into the bloodstream, reaching the heart, brain, and other organs. The WHO recognises PM2.5 as the single most health-relevant component of outdoor air pollution.
Ultrafine particles (PM0.1, ≤0.1 micrometres) are increasingly studied and may be even more biologically active per unit mass than PM2.5, though measurement and regulation of this fraction is less established.
Gaseous Pollutants
Nitrogen dioxide (NO₂) is produced primarily by combustion engines and industrial processes. It inflames the airways, reduces ciliary function (the tiny hair-like structures that sweep debris out of the lungs), and increases susceptibility to respiratory infections. People with asthma are particularly sensitive to NO₂.
Sulfur dioxide (SO₂) originates mainly from burning coal and heavy fuel oil. It causes bronchoconstriction — airway narrowing — and is a potent trigger for asthma attacks even at relatively low concentrations.
Ground-level ozone (O₃) is formed when sunlight reacts with vehicle exhaust and industrial emissions. It is a powerful oxidant that damages the lung’s epithelial cells, causing inflammation, reduced lung function, and worsened asthma. Ozone concentrations are often highest on hot, sunny days — when people are most likely to be outdoors.
Carbon monoxide (CO) binds to haemoglobin with 200 times greater affinity than oxygen, reducing the blood’s oxygen-carrying capacity. At high concentrations, it is acutely dangerous; at chronic low levels, it contributes to cardiovascular and respiratory strain.
Indoor Pollutants
Indoor air quality is frequently overlooked but critically important. The EPA has estimated that indoor air can be two to five times more polluted than outdoor air in some settings. Key indoor pollutants include:
- Biomass and solid fuel combustion: Cooking and heating with wood, charcoal, coal, or crop residues produces intense concentrations of PM2.5, CO, and volatile organic compounds (VOCs). This is the primary exposure source for a substantial portion of the global population.
- Tobacco smoke: Both primary and secondhand smoke contain over 7,000 chemical compounds, many of which are directly toxic to lung tissue.
- Volatile organic compounds (VOCs): Off-gassed from paints, adhesives, cleaning products, and synthetic furnishings. Benzene, formaldehyde, and toluene are among the more harmful examples.
- Radon: A naturally occurring radioactive gas that seeps from soil and rock into buildings. The second leading cause of lung cancer after smoking in several countries.
- Biological pollutants: Mould spores, dust mite faeces, and pet dander trigger allergic airway inflammation and worsen asthma.
How Pollution Damages the Lungs: The Mechanisms
Understanding how pollution harms lung tissue — not just that it does — is important for understanding why the damage accumulates silently and why prevention is so much more effective than treatment.
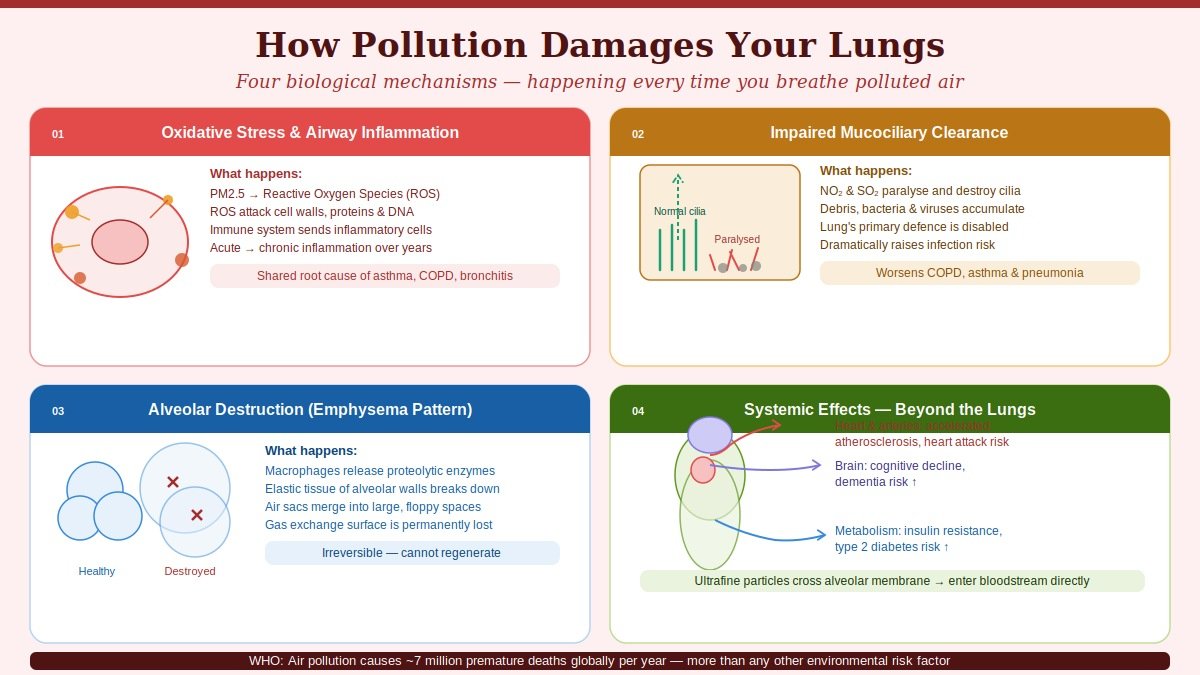
1. Oxidative Stress and Airway Inflammation
When PM2.5 and gaseous pollutants reach the airway lining, they trigger the production of reactive oxygen species (ROS) — unstable molecules that attack cell membranes, proteins, and DNA. The immune system responds by sending inflammatory cells to the site, releasing cytokines (inflammatory signalling molecules) and initiating an inflammatory cascade.
In the short term, this produces the familiar symptoms of irritation: coughing, mucus production, and airway constriction. In the long term — with daily pollutant exposure — the inflammation becomes chronic. Chronic airway inflammation is the shared underlying mechanism in asthma, COPD, and chronic bronchitis. It damages the structural integrity of the airway wall and, over time, promotes the fibrotic (scarring) changes seen in advanced respiratory disease.
2. Impaired Mucociliary Clearance
The airways are lined with millions of tiny hair-like projections called cilia, which beat in coordinated waves to sweep inhaled debris, pathogens, and mucus toward the throat, where it can be swallowed or coughed out. This mucociliary escalator is the lung’s primary mechanical defence.
Pollutants — particularly NO₂, SO₂, and cigarette smoke — paralyse and eventually destroy cilia. With impaired clearance, inhaled particles, bacteria, and viruses accumulate in the airways instead of being expelled, dramatically increasing the risk of respiratory infections, exacerbations of chronic disease, and progressive airway damage.
3. Alveolar Destruction
The alveoli — the tiny air sacs where oxygen crosses into the bloodstream — are exquisitely sensitive to oxidative injury. PM2.5 particles that reach this level trigger macrophage activation (alveolar macrophages are the immune cells that patrol the deep lung), which releases further inflammatory mediators and proteolytic enzymes. Over time, these enzymes break down the elastic tissue of the alveolar walls — the same pathological process that produces emphysema in smokers, and that chronic pollution exposure can accelerate.
Lost alveolar surface area cannot be recovered. Once destroyed, those gas exchange units are gone permanently.
4. Systemic Effects: Beyond the Lungs
The lung is a gateway, not a barrier. Ultrafine particles and the inflammatory mediators triggered by pollutant exposure are not confined to the respiratory tract. They enter the bloodstream, contributing to:
- Cardiovascular disease: Systemic inflammation and direct particle deposition in vessel walls accelerate atherosclerosis and increase risk of heart attack and stroke
- Neurological effects: Emerging evidence links long-term PM2.5 exposure to cognitive decline and increased risk of dementia
- Metabolic disruption: Pollution exposure is associated with increased insulin resistance and type 2 diabetes risk
- Adverse pregnancy outcomes: Preterm birth, low birth weight, and impaired foetal lung development are linked to gestational pollution exposure
How Pollution Affects Lung Development in Children
Children are not simply small adults in the context of pollution exposure. Their lungs are actively developing from before birth through early adulthood — a process that continues until approximately age 25. During this window, the lung’s architecture is being built: airways are branching, alveoli are multiplying, and the elastic tissue framework is being established.
Pollution disrupts this process in ways that cannot always be remediated later:
Reduced lung growth: Landmark research, including the Children’s Health Study in the United States, demonstrated that children who grew up in higher-pollution areas had measurably smaller lungs — lower FVC and FEV1 — than peers in cleaner environments. These deficits persisted into adulthood.
Earlier onset of respiratory disease: Children with high pollution exposure are significantly more likely to develop asthma, recurrent lower respiratory infections, and bronchial hyperreactivity. Each severe respiratory infection in early childhood, particularly those requiring hospitalisation, is associated with increased risk of COPD in adulthood.
Cognitive impacts: Fine particle exposure in childhood is associated with reduced cognitive development, attention deficits, and lower educational attainment — outcomes mediated both by direct neurological effects and by the chronic ill-health that pollution-related respiratory disease causes.
This is why WHO guidelines for PM2.5 place particular emphasis on protecting children, and why paediatric respiratory health is disproportionately affected in high-pollution communities globally.
Pollution and Respiratory Disease: The Disease-Specific Picture
Asthma
Air pollution both triggers acute asthma attacks and, with long-term exposure, increases the risk of developing asthma in the first place. Ozone and NO₂ are the primary attack triggers; PM2.5 drives the underlying sensitisation and airway hyperreactivity. On high-pollution days, emergency department admissions for acute asthma reliably increase — a pattern documented across cities on every inhabited continent.
COPD
Long-term exposure to PM2.5 and occupational dusts is the second leading cause of COPD globally after cigarette smoking. Biomass fuel combustion — still used for cooking and heating by billions of people, primarily in lower- and middle-income countries — is responsible for a substantial share of COPD in non-smoking women worldwide. Critically, many of these cases go undiagnosed for years: the slow onset of breathlessness is dismissed as ageing, and spirometry is unavailable or not offered.
Lung Cancer
The International Agency for Research on Cancer (IARC) classified outdoor air pollution, and PM2.5 specifically, as Group 1 human carcinogens in 2013 — meaning the evidence that they cause cancer in humans is unequivocal. Globally, air pollution is estimated to account for approximately 15% of all lung cancer deaths.
Interstitial Lung Disease and Pulmonary Fibrosis
Chronic occupational and environmental PM exposure is a recognised cause of interstitial lung diseases, including occupational forms of pulmonary fibrosis. The mechanism involves sustained macrophage activation and progressive deposition of collagen in the interstitium — the tissue framework of the lung — reducing its elasticity and gas exchange capacity.
Respiratory Infections
Beyond chronic disease, polluted air makes acute infections more likely and more severe. Influenza, pneumonia, and COVID-19 all have worse outcomes in populations with higher pollution exposure — both because impaired mucociliary clearance allows pathogens easier access to the deep lung, and because chronic inflammation compromises the immune response to acute infection.
Warning Signs That Pollution May Be Affecting Your Lungs
The insidious nature of pollution-related lung damage is that it is largely asymptomatic until significant harm has occurred. However, several symptoms warrant medical evaluation, particularly if they correlate with high-pollution periods:
- Persistent or worsening cough — especially a productive cough, or one that worsens in winter or on high-pollution days
- Progressive breathlessness — initially on exertion, but advancing to breathlessness at rest over time
- Chest tightness — particularly in the morning or after outdoor activity
- Recurrent respiratory infections — more than two or three chest infections per year should prompt investigation
- Reduced exercise tolerance — finding activities significantly harder than they used to be, without other obvious cause
- Wheezing — particularly episodic or in response to environmental change
- Fatigue — often an underappreciated symptom of reduced lung function and oxygen efficiency
Important: Symptoms that are present at rest, that limit daily activities, or that are worsening over weeks despite avoiding obvious triggers require prompt medical assessment. SpO2 monitoring at home (a pulse oximeter provides readings in seconds) is a practical early warning tool — persistent readings below 95% at rest warrant professional evaluation.
Who Is Most Vulnerable
While air pollution affects everyone, certain populations face disproportionately higher risk of serious harm:
Children (especially under 5): Developing lung architecture, higher respiratory rate relative to body weight (meaning proportionally more air — and pollutants — inhaled per kg), and developing immune systems combine to make young children the most vulnerable population.
Elderly adults: Reduced respiratory reserve, declining immune function, and the higher prevalence of pre-existing cardiovascular and respiratory disease increase the severity of pollution-related harm in older adults.
People with existing respiratory or cardiovascular disease: Every major respiratory condition — asthma, COPD, bronchiectasis, pulmonary fibrosis — is exacerbated by pollution exposure. The threshold for triggering a flare-up is dramatically lower in these individuals.
Pregnant women: The developing foetus is highly sensitive to placental oxidative stress, and systemic inflammation from maternal pollution exposure is associated with adverse birth outcomes.
Outdoor workers: Construction workers, traffic police, delivery workers, agricultural labourers — anyone whose livelihood requires extended outdoor time in polluted environments faces significantly higher cumulative exposure.
People of lower socioeconomic status: Disproportionately likely to live near pollution sources, less likely to have access to filtered indoor air, less likely to be able to work remotely on high-pollution days, and often with less access to preventive healthcare.
Evidence-Based Protection Strategies
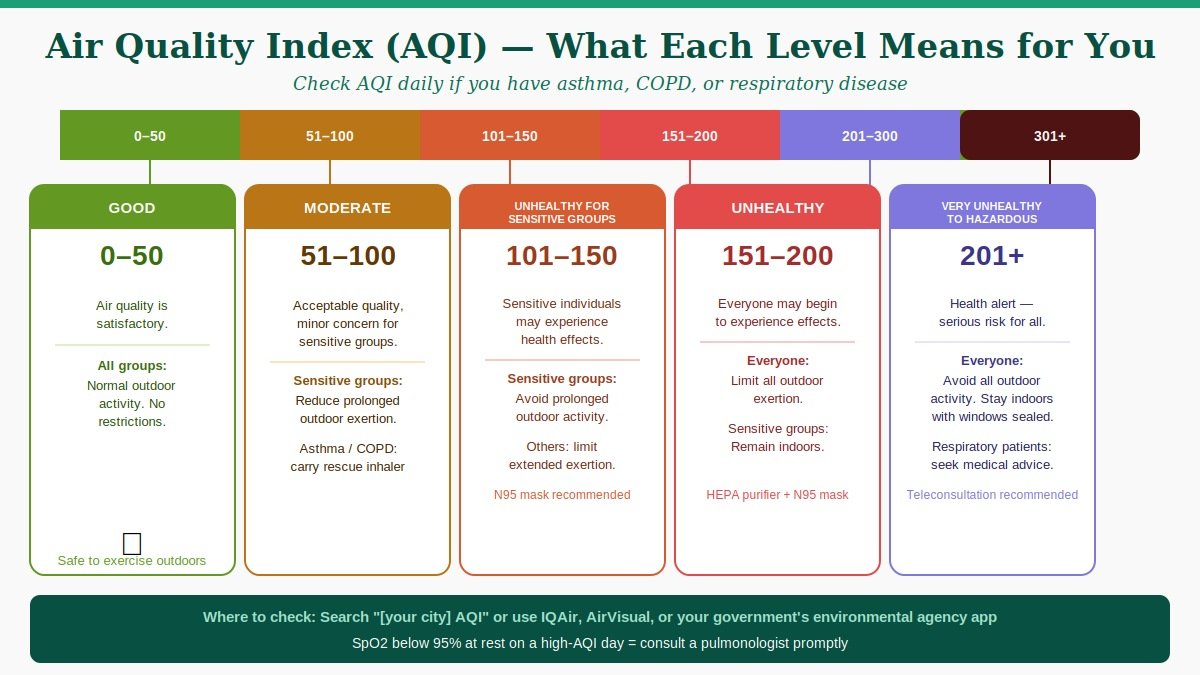
1. Monitor the Air Quality Index (AQI)
Real-time AQI data is available in most countries via government environmental agencies or weather apps. Understanding what the numbers mean in practical terms:
- AQI 0–50 (Good): No restriction on outdoor activity
- AQI 51–100 (Moderate): Sensitive individuals (asthma, COPD, children, elderly) should reduce prolonged outdoor exertion
- AQI 101–150 (Unhealthy for Sensitive Groups): Sensitive groups should avoid prolonged outdoor activity; others should reduce it
- AQI 151–200 (Unhealthy): Everyone should limit outdoor exertion; sensitive groups should remain indoors
- AQI 201+ (Very Unhealthy / Hazardous): All outdoor activity should be minimised
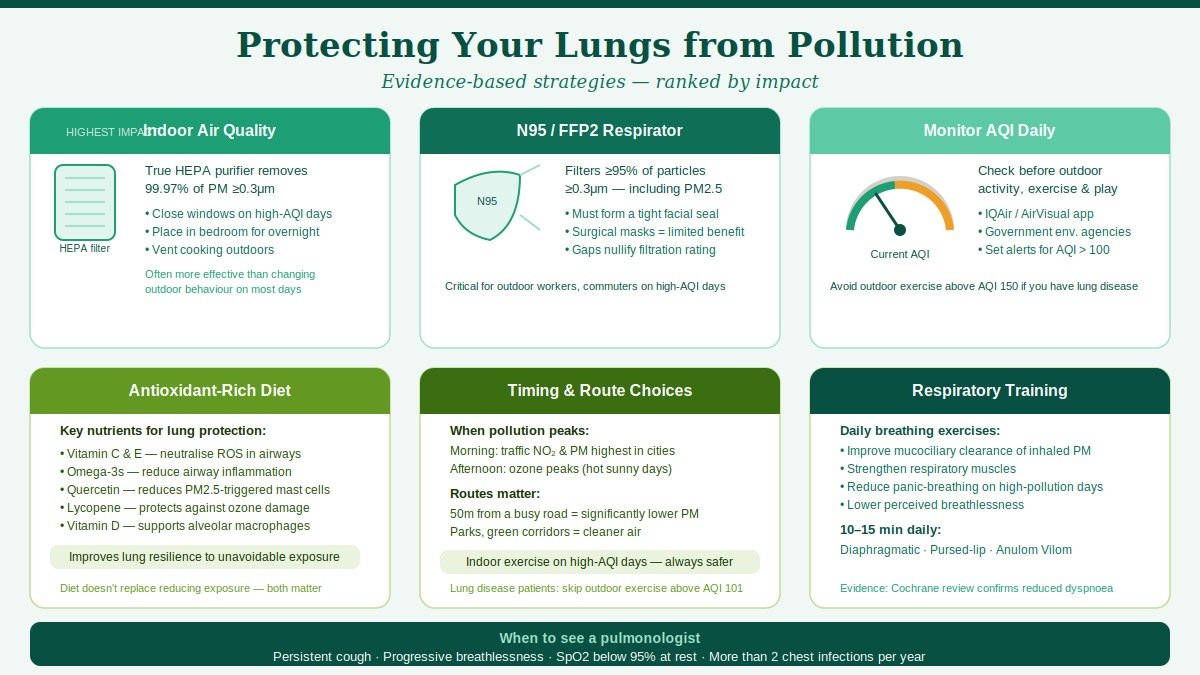
2. Respiratory Protection: Masks
Not all masks offer equal protection against PM2.5. Standard surgical masks and cloth masks provide minimal filtration of fine particles. N95/FFP2 respirators (when properly fitted — no gaps at the seal) filter at least 95% of airborne particles ≥0.3 micrometres. For regular high-pollution commuting or outdoor work, these are the minimum standard worth wearing.
Fit matters as much as filtration rating — an N95 worn loosely, with gaps at the cheeks or nose bridge, provides substantially less protection than its rating suggests.
3. Indoor Air Quality Management
Given how much time most people spend indoors, indoor air quality management often provides more total exposure reduction than outdoor behaviour changes.
HEPA filtration: True HEPA air purifiers (filtering particles ≥0.3 micrometres at 99.97% efficiency) significantly reduce indoor PM2.5 levels. Room-size purifiers should be matched to the volume of the space; multiple units are often needed for full home coverage. Place units in the rooms where you spend the most time — bedroom overnight is particularly valuable.
Ventilation strategy: On high-AQI days, keeping windows closed and running an air purifier reduces indoor PM2.5 far more effectively than ventilating with outdoor air. On low-AQI days — particularly in the morning before traffic peaks — opening windows for ventilation improves overall air quality.
Eliminating indoor sources: Cooking without adequate ventilation, candles and incense, aerosol sprays, harsh cleaning chemicals, and volatile furniture finishes are all meaningful sources of indoor PM and VOC exposure. Range hoods vented to the outside are one of the most impactful indoor interventions available.
Houseplants: While popular, the evidence for meaningful air purification by indoor plants is weak — the quantities needed to produce measurable PM reduction are impractical in residential settings. HEPA filtration is substantially more effective.
4. Respiratory Muscle Training
Regular breathing exercises — particularly diaphragmatic breathing and pursed-lip breathing — improve the mechanical efficiency of the lung, enhance mucociliary clearance, and strengthen the respiratory muscles that compensate for pollution-related airway narrowing. These are not merely wellness practices; they are evidence-backed, recommended by respiratory physiotherapists as part of management plans for pollution-exposed individuals with chronic respiratory disease.
5. Nutritional Support for Lung Health
The lung is exceptionally vulnerable to oxidative stress because of its continuous exposure to oxygen and airborne oxidants. Dietary antioxidants provide meaningful — though not complete — protection:
Vitamin C and E: Powerful antioxidants that neutralise ROS in the airway lining fluid. Found in citrus fruits, berries, bell peppers, nuts, and seeds.
Omega-3 fatty acids: Anti-inflammatory effects that may reduce the airway inflammation triggered by pollution. Found in oily fish, flaxseed, and walnuts. A Cochrane review found that omega-3 supplementation reduced airway inflammation markers in asthma patients.
Quercetin and flavonoids: Found in onions, apples, green tea, and dark leafy vegetables. Evidence suggests quercetin specifically reduces mast cell activation triggered by PM2.5.
Vitamin D: Deficiency is associated with worse respiratory outcomes in multiple studies; adequate vitamin D supports the immune surveillance function of the lung’s alveolar macrophages.
Lycopene: The red-orange pigment in tomatoes and watermelon is concentrated in lung tissue and appears to offer specific protection against ozone-related oxidative damage.
6. Reduce Personal Emission Contributions
Individual choices that reduce contribution to ambient pollution also reduce collective exposure: avoiding diesel vehicles, choosing lower-emission transportation where available, reducing open burning, and improving home heating efficiency all reduce the ambient pollution that everyone — including yourself — breathes.
7. Timing and Route Choices
On high-pollution days, the timing and route of outdoor activity matters:
- Early morning is often highest in traffic-related NO₂ and particulates in urban areas; midday can be highest in ozone (when sunlight is strongest)
- Avoid major road routes for exercise or walking; even a 50-metre set-back from a busy road significantly reduces PM exposure
- Exercising outdoors in high-pollution conditions is net harmful for people with respiratory disease — the increased ventilation of exercise brings proportionally more pollutants into the deep lung. On high-AQI days, indoor exercise is categorically preferable
The Global Burden: Why This Matters
The WHO estimates that ambient (outdoor) air pollution causes approximately 4.2 million premature deaths annually. Combined with household air pollution deaths, the total exceeds 7 million — making air pollution the world’s largest environmental health risk factor, ahead of unsafe water, poor sanitation, or any single infectious disease other than COVID-19 at peak pandemic.
This burden is not evenly distributed. Low- and middle-income countries account for approximately 90% of air pollution deaths, driven by higher ambient pollution levels, greater reliance on solid fuels for cooking and heating, lower access to healthcare for early diagnosis and management, and less political and economic capacity to enforce emissions regulations.
But high-income countries are not insulated. Urban air quality remains a significant health concern across Europe, North America, and Australia. The UK Health Security Agency estimates that long-term exposure to outdoor air pollution contributes to approximately 28,000 to 36,000 deaths annually in England alone. The economic cost of air pollution — in healthcare expenditure, lost productivity, and premature mortality — runs to trillions of dollars globally.
When to See a Pulmonologist
The general practitioner is often the appropriate first contact for mild respiratory symptoms. However, several situations specifically warrant a respiratory specialist:
- Chronic cough lasting more than 8 weeks without an identified cause
- Breathlessness that limits activity or is worsening over weeks to months
- Spirometry abnormality identified at a GP visit or health screening
- Recurrent chest infections — more than two per year requiring antibiotics or steroids
- Asthma that is not well-controlled on standard therapy
- Diagnosis uncertain — symptoms overlap between multiple conditions (asthma, COPD, vocal cord dysfunction, cardiac breathlessness)
- Occupational exposure history — anyone with significant past or current exposure to occupational dusts, chemicals, or fumes should have baseline spirometry and regular review
- Smoking history of 20+ pack-years — eligibility for low-dose CT lung cancer screening in many guidelines
A key message for anyone living or working in a high-pollution environment: don’t normalise breathlessness. The progressive nature of pollution-related lung disease means that by the time symptoms are clearly limiting, substantial irreversible damage has often occurred. Earlier evaluation preserves more options.
FAQs
Q1: Can pollution cause permanent lung damage? Yes. The destruction of alveolar tissue (as in emphysema-pattern COPD) is permanent — lost gas exchange surface cannot regenerate. Fibrotic changes from chronic inflammation are also largely irreversible. However, reducing exposure at any point slows further damage and, particularly in younger individuals, allows for some recovery of airway inflammation and mucociliary function. Early intervention significantly changes the trajectory.
Q2: Are N95 masks effective against PM2.5? When properly fitted — with a tight seal at the nose and cheeks — yes. Properly worn N95/FFP2 respirators filter at least 95% of PM2.5. The key limitation is fit: gaps in the seal substantially reduce protection. For people with beards or unusual face shapes, fit-testing is valuable. Standard surgical masks offer limited protection against fine particles.
Q3: Is indoor air always safer than outdoor air? Not necessarily. Indoor air quality depends heavily on the presence of indoor sources (cooking smoke, tobacco, VOCs), the building’s ventilation system, and whether any outdoor air filtration is in place. In homes with solid fuel cooking, indoor PM2.5 concentrations can exceed even the most polluted outdoor environments. In well-sealed buildings with HEPA filtration, indoor air can be substantially cleaner than outdoor air even on high-pollution days.
Q4: At what age does pollution damage become irreversible? There is no clear threshold. Damage accumulates throughout life, and the lung has meaningful repair capacity for mild to moderate inflammatory injury — particularly in younger people. However, alveolar destruction and fibrotic changes are irreversible at any age. This is why reducing exposure earlier in life produces the greatest long-term benefit. Children with persistent high-pollution exposure during lung development may carry that deficit permanently.
Q5: Can diet meaningfully protect against pollution-related lung damage? Diet is not a substitute for reducing exposure, but it does provide meaningful biological protection. The antioxidant-rich dietary pattern — high in colourful vegetables and fruits, oily fish, nuts, and green tea — corresponds closely to what the evidence supports for reducing pollution-related inflammatory damage. Think of it as improving the lung’s ability to handle unavoidable exposure, not eliminating the exposure itself.
Q6: Does moving to a less polluted area improve lung health? Yes. Multiple studies have followed populations that moved from high-pollution to lower-pollution areas and documented measurable improvements in lung function, reductions in inflammatory markers, and lower rates of respiratory exacerbations. In children, relocation during the developmental window appears to partially reverse pollution-related lung growth deficits. The benefit is real, though not complete — some irreversible damage remains.
Conclusion: An Invisible Crisis That Demands a Visible Response
Air pollution is not an abstract environmental statistic. It is a daily biological event happening inside your airways, at the cellular level, with consequences that accumulate silently over years and decades. By the time symptoms become undeniable, lung function that could have been preserved may already be lost.
The most powerful protection is reducing exposure — monitoring AQI, using appropriate respiratory protection, managing indoor air quality, and making choices that reduce both personal exposure and collective emissions. For people with existing respiratory disease, regular specialist review is essential: pollution worsens every major lung condition, and management plans need to account for the environmental exposures patients face every day.
Breathing is the body’s most fundamental act — roughly 22,000 times per day. It deserves more attention than most of us give it.

