Breathing problems can feel deceptively similar from the inside. But the conditions causing them are worlds apart.
You wake up at 2 a.m. struggling to breathe. Or you’ve had a cough that won’t quit for the past three weeks. Or you notice that climbing a flight of stairs leaves you winded in a way it never used to.
These experiences might point to asthma. They might indicate COPD. Or they could signal bronchitis — or even some combination of all three.
Respiratory conditions are among the most common — and most misunderstood — health problems worldwide. Millions of people live with a diagnosis they don’t fully understand, using medications that don’t quite fit, or delaying care because they assume their symptoms are “just a cough.” In a country like India, where air quality is a daily concern for hundreds of millions of people, the stakes are even higher.
This guide breaks down the real differences between asthma, COPD, and bronchitis: how they develop, how they feel, how they’re diagnosed, and — critically — how they’re treated differently.
A Quick Snapshot: Three Conditions, Three Different Stories
Before diving deep, here’s the high-level picture:
| Feature | Asthma | COPD | Bronchitis |
|---|---|---|---|
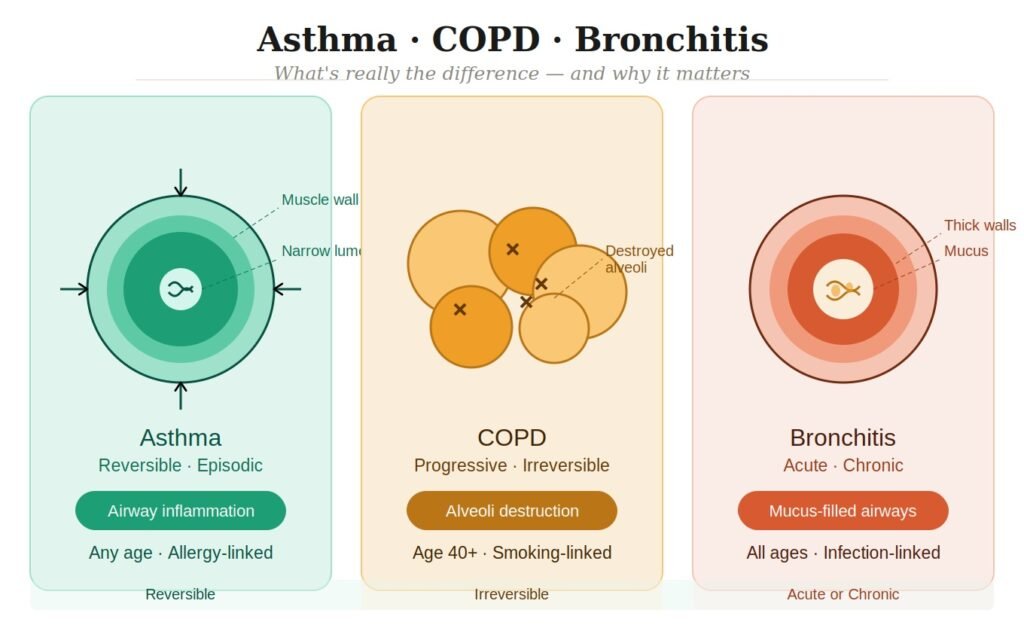
| Nature | Reversible (with treatment) | Progressive, largely irreversible | Acute or chronic |
| Primary Cause | Allergic triggers, airway hyperreactivity | Long-term smoking, pollution exposure | Viral/bacterial infection or irritant exposure |
| Typical Age of Onset | Childhood or young adulthood | Usually after age 40 | Any age |
| Core Symptom | Episodic wheezing & breathlessness | Persistent, worsening breathlessness | Productive cough with mucus |
| Airflow Obstruction | Intermittent | Constant and progressive | Temporary (acute) or constant (chronic) |
| Reversibility | Largely reversible | Not fully reversible | Acute: fully reversible |
| Prognosis with Treatment | Very manageable | Manageable but progressive | Acute resolves; chronic requires ongoing care |
What Is Asthma? A Deeper Look
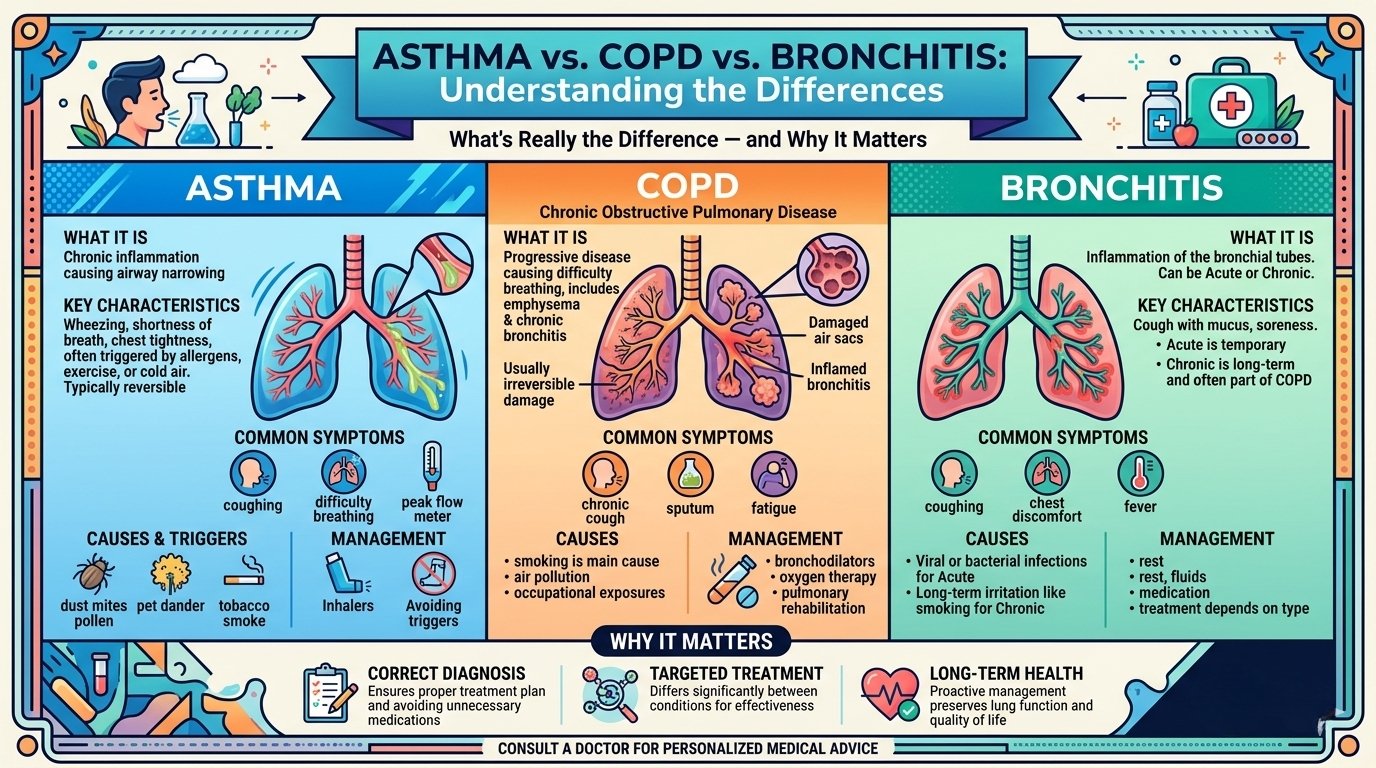
Asthma is a chronic inflammatory disease of the airways. At its core, it involves three overlapping problems: airway inflammation, bronchoconstriction (tightening of the muscles around the airways), and increased mucus production. Together, these make the airways narrow and difficult to breathe through.
What makes asthma distinct from other respiratory conditions is its episodic, reversible nature. Between attacks or flare-ups, many people with asthma have completely normal breathing. The airways can open and close dramatically depending on exposure to triggers.
Who Gets Asthma?
Asthma is one of the few respiratory conditions that affects children and adults equally. It often first appears in childhood, though adult-onset asthma is common. It has a strong genetic component — if one parent has asthma, a child’s risk increases significantly. It’s also closely linked with other allergic conditions: eczema, hay fever, and food allergies often travel together with asthma in the same individual or family. This constellation is called the “atopic triad.”
In India, asthma affects an estimated 30 million people. Urban children in cities with high pollution loads — Delhi, Mumbai, Kolkata — face a disproportionately higher burden.
Symptoms of Asthma
- Wheezing — a high-pitched whistling sound when breathing, especially exhaling
- Shortness of breath — often episodic, worse during exercise or at night
- Chest tightness — a feeling of pressure or squeezing in the chest
- Coughing — frequently worse at night or early morning; sometimes a dry cough is the only symptom (cough-variant asthma)
Common Asthma Triggers
Triggers vary between individuals, but the most common include:
- Allergens: dust mites, pet dander, pollen, mould
- Air quality: smoke, vehicle exhaust, industrial pollution, incense smoke (highly relevant in Indian households)
- Infections: respiratory viruses, especially in children
- Exercise: exercise-induced bronchoconstriction is common
- Weather: cold air, sudden temperature changes, high humidity
- Emotional stress and strong emotions
- Certain medications: aspirin and NSAIDs in some individuals (aspirin-exacerbated respiratory disease)
How Asthma Progresses
With good management, asthma doesn’t have to worsen over time. However, poorly controlled asthma causes repeated cycles of inflammation that can, over years, permanently remodel the airway walls — a process called airway remodelling. This is why early, consistent treatment matters. What starts as a fully reversible condition can cause lasting structural changes if neglected for years.
What Is COPD? A Deeper Look
Chronic Obstructive Pulmonary Disease (COPD) is an umbrella term for a group of progressive lung diseases that cause permanently obstructed airflow. It’s not one disease but a spectrum, primarily comprising:
- Emphysema: the air sacs (alveoli) at the end of the airways are progressively destroyed, reducing the surface area for oxygen exchange. Imagine a healthy lung as millions of tiny grapes — emphysema turns them into large, floppy balloons that can’t push air out effectively.
- Chronic bronchitis: long-term inflammation of the bronchial tubes, producing persistent cough and excess mucus production for at least three months in two consecutive years. This is often the “productive cough” component of COPD.
Most people with COPD have elements of both.
What Causes COPD?
In high-income countries, cigarette smoking accounts for approximately 85–90% of COPD cases. In India and other parts of Asia, however, the picture is more complex:
- Biomass fuel exposure: Cooking over wood, dung, or crop-residue fires in poorly ventilated kitchens — still common in rural India — exposes women and children to toxic particle concentrations. Studies show this is responsible for a significant share of COPD in non-smoking Indian women.
- Occupational dust and chemicals: Grain dust, coal dust, silica, and chemical fumes cause occupational COPD.
- Outdoor air pollution: Long-term exposure to high PM2.5 concentrations accelerates lung function decline.
- Childhood lung infections: Severe pneumonia in childhood can stunt lung development and predispose someone to COPD decades later.
- Alpha-1 antitrypsin deficiency: A genetic condition where the lungs lack a protective enzyme, causing early-onset COPD even without smoking.
Symptoms of COPD
COPD symptoms develop slowly and insidiously, which is why many people dismiss them for years:
- Progressive breathlessness: Initially only on exertion; over time, at rest. This is the hallmark.
- Chronic cough: Often productive (mucus-producing), present most days
- Increased mucus (sputum) production: Especially in the mornings
- Frequent chest infections: Lungs compromised by COPD are more vulnerable to infections, which in turn worsen COPD — a vicious cycle
- Fatigue and reduced exercise tolerance
- Wheezing and chest tightness (overlaps with asthma)
- In advanced stages: Barrel-shaped chest, cyanosis (blue tinge to lips/fingers), and weight loss
The GOLD Staging System
COPD severity is measured by the GOLD (Global Initiative for Chronic Obstructive Lung Disease) classification, using spirometry results and symptom burden:
- GOLD 1 (Mild): Some airflow limitation; often no symptoms yet
- GOLD 2 (Moderate): Worsening airflow; shortness of breath on exertion
- GOLD 3 (Severe): Significant airflow limitation; daily activities affected
- GOLD 4 (Very Severe): Very limited airflow; reduced quality of life and risk to life
Early diagnosis is crucial — by the time most people seek care, they have already lost 50% or more of their lung function.
What Is Bronchitis? A Deeper Look
Bronchitis is inflammation of the bronchial tubes — the large airways that carry air to and from the lungs. It’s important to understand that bronchitis is not a single disease but rather a symptom pattern that can arise from very different underlying causes.
Acute Bronchitis
Acute bronchitis is extremely common — most people will experience it at least once in their lives. It’s almost always caused by a viral infection (rhinovirus, influenza, RSV, adenovirus), following a cold or respiratory infection. Bacterial causes are less common but possible.
Key features:
- Develops over days
- Productive cough — initially dry, then mucus-producing (mucus may appear yellow or green, which doesn’t always indicate bacterial infection)
- Often preceded by a sore throat, runny nose, or cold symptoms
- Low-grade fever and fatigue
- Chest soreness from coughing
- Typically resolves within 1–3 weeks
Antibiotics are usually not needed for acute bronchitis, as it’s almost always viral. Overuse of antibiotics for acute bronchitis is a significant contributor to antibiotic resistance in India.
Chronic Bronchitis
Chronic bronchitis is a very different beast — it’s the long-term, structural form. Officially defined as a productive cough lasting at least 3 months per year for 2 or more consecutive years, chronic bronchitis is usually caused by:
- Cigarette smoking (the most common cause)
- Prolonged exposure to air pollutants or occupational irritants
- Recurrent respiratory infections in childhood that permanently impair airway defenses
Chronic bronchitis is, by definition, part of COPD. When a smoker develops chronic bronchitis, it signals that COPD is likely present or developing.
Chronic bronchitis is not a temporary illness — it is a chronic disease requiring long-term management.
The Key Differences, Explained in Plain Terms
1. Reversibility: Can Your Airways Open Back Up?
This is perhaps the most clinically important distinction.
Asthma is characterised by reversible airway obstruction. Give a person with asthma a bronchodilator inhaler and their spirometry (breathing test) numbers can jump dramatically — sometimes returning fully to normal within minutes. The airways close, but they can open again.
COPD involves largely irreversible airway obstruction. The destruction of lung tissue (emphysema) and structural changes to the airways cannot be undone. Bronchodilators help open what can be opened, but the underlying damage persists. There is no “recovering” full lung function once it’s lost in COPD.
Bronchitis (acute) is fully reversible — the inflammation resolves and the airways return to baseline. Chronic bronchitis, however, shares the irreversibility of COPD.
2. The Type of Breathing Difficulty
- Asthma: Episodic breathlessness. Normal days punctuated by attacks. Often worse at night or in the morning.
- COPD: Constant, progressive breathlessness that gradually worsens over years. “Never quite getting a full breath.”
- Acute bronchitis: Breathlessness tied to active infection; chest feels congested. Resolves with the illness.
3. The Inflammatory Process
The inflammation in asthma is primarily eosinophilic (driven by immune cells called eosinophils, linked to allergy). In COPD, it’s predominantly neutrophilic and macrophage-driven — the type of inflammation triggered by toxic particles and smoke, not by allergens. This distinction matters because it means different medications target different pathways.
4. Response to Steroids
Asthma responds strongly to inhaled corticosteroids (ICS) — they are the cornerstone of asthma treatment.
COPD responds much less robustly to steroids, though they have a role in certain subtypes (especially those with overlapping asthma features).
This difference is clinically significant: a doctor who can’t distinguish asthma from COPD may over-prescribe steroids for COPD patients or under-prescribe them for asthma patients.
5. Who Is at Risk
| Asthma | COPD | Bronchitis | |
|---|---|---|---|
| Children | Common | Rare | Common (acute) |
| Young adults | Yes | Uncommon | Yes |
| Smokers | Not specifically | Very high risk | High risk (chronic) |
| People with allergies | Very high risk | No specific link | Moderate |
| Pollution exposure | Yes (triggers) | Yes (cause) | Yes (cause and trigger) |
The Asthma-COPD Overlap (ACO): When Things Get Complicated
Medicine is rarely clean-cut. A significant portion of patients — estimated at 15–25% of those with obstructive lung disease — have features of both asthma and COPD simultaneously. This is called Asthma-COPD Overlap (ACO).
ACO typically presents in:
- Older adults who had asthma since childhood and smoked for years
- People with asthma who developed fixed airway obstruction due to airway remodelling
- Smokers with COPD who also show significant bronchodilator reversibility and eosinophilic inflammation
ACO patients tend to have:
- More frequent exacerbations than COPD alone
- Worse quality of life
- A better response to inhaled corticosteroids than “pure” COPD
This overlap is exactly why self-diagnosis and generic treatment don’t work — accurate differentiation requires a pulmonologist, spirometry, and often additional tests.
How Are These Conditions Diagnosed?
Spirometry: The Gold Standard
Spirometry is the cornerstone of diagnosing all three conditions. The patient breathes into a device that measures:
- FVC (Forced Vital Capacity): Total air breathed out forcefully
- FEV1 (Forced Expiratory Volume in 1 second): How much air is expelled in the first second
- FEV1/FVC ratio: A ratio below 0.70 indicates airflow obstruction
Crucially, a bronchodilator reversibility test is performed: the patient is given a short-acting bronchodilator, and spirometry is repeated after 15–20 minutes. A significant improvement (≥12% and ≥200ml increase in FEV1) suggests asthma rather than COPD.
Additional Diagnostic Tools
- Peak flow monitoring: Daily measurements with a peak flow meter can reveal the variability in airflow characteristic of asthma
- FeNO test (Fractional exhaled Nitric Oxide): Elevated FeNO indicates eosinophilic airway inflammation — pointing toward asthma
- Chest X-ray: May show hyperinflation in COPD; can rule out pneumonia in bronchitis
- High-resolution CT scan: Best tool for visualizing emphysema; can identify bronchiectasis
- Allergy testing (skin prick test / IgE blood tests): Identifies allergic triggers in asthma
- Blood tests: Eosinophil count, Alpha-1 antitrypsin levels, CBC to check for infection
- Sputum analysis: To identify infective organisms in bronchitis or COPD exacerbations
- Pulse oximetry and arterial blood gas: Assesses oxygen levels, especially in severe disease
Treatment: Why “One Size Fits All” Fails
Treating Asthma
The goal of asthma treatment is complete control — no daytime symptoms, no night waking, no limitation of activity, no exacerbations.
Inhaled Corticosteroids (ICS) are the backbone — they reduce airway inflammation. Common examples: budesonide, fluticasone, beclomethasone.
Short-acting beta-2 agonists (SABAs) like salbutamol (albuterol) are “rescue inhalers” — used during acute episodes to rapidly open the airways.
Long-acting beta-2 agonists (LABAs) like formoterol or salmeterol are added when ICS alone don’t provide adequate control. They’re always combined with ICS in asthma.
Leukotriene receptor antagonists (LTRAs) like montelukast are oral medications that reduce allergic inflammation, often used alongside inhalers.
Biologics: For severe, difficult-to-control asthma, newer injectable biologic medications target specific inflammatory pathways:
- Omalizumab (anti-IgE) for allergic asthma
- Mepolizumab, benralizumab (anti-IL-5) for eosinophilic asthma
- Dupilumab (anti-IL-4/IL-13) for type-2 inflammation
Trigger avoidance is non-negotiable and just as important as medication.
Treating COPD
COPD treatment focuses on slowing progression, reducing symptoms, preventing exacerbations, and improving quality of life — not curing the disease.
Long-acting bronchodilators are the cornerstone:
- LABAs (long-acting beta-2 agonists): formoterol, salmeterol, indacaterol
- LAMAs (long-acting muscarinic antagonists): tiotropium, glycopyrronium, umeclidinium
- Dual LABA+LAMA combinations are often preferred
Inhaled corticosteroids are added selectively — in patients with frequent exacerbations or elevated eosinophil counts, not routinely for all COPD patients.
Pulmonary rehabilitation — a structured programme of exercise, breathing techniques, and education — is one of the most effective interventions for improving exercise capacity and quality of life. It’s underutilized in India.
Smoking cessation is the single most important intervention. No medication matches the benefit of stopping smoking in terms of slowing disease progression.
Long-term oxygen therapy for patients with chronically low oxygen levels (SpO2 <88%)
Vaccinations: Influenza annually, pneumococcal vaccine — respiratory infections can cause life-threatening COPD exacerbations.
Surgical options in select severe cases: lung volume reduction surgery, bullectomy, or lung transplantation.
Treating Bronchitis
Acute bronchitis is mostly self-limiting. Treatment focuses on symptom relief:
- Rest and adequate hydration (helps thin mucus)
- Honey and ginger (evidence-supported home remedies for cough)
- Over-the-counter cough suppressants or expectorants for symptom comfort
- Antipyretics for fever
- Antibiotics are NOT recommended unless there is clear evidence of bacterial infection (which is uncommon) or the patient is high-risk (COPD, immunocompromised, elderly)
- In patients with underlying asthma, a short course of bronchodilators may be helpful if wheezing is present
Chronic bronchitis treatment overlaps with COPD management:
- Smoking cessation above everything else
- Bronchodilators
- Pulmonary rehabilitation
- Management of exacerbations (which do require antibiotics when bacterial)
- Mucolytics (e.g., carbocisteine, NAC) to reduce mucus thickness
India-Specific Context: Why This Is a Public Health Emergency
India carries one of the world’s largest burdens of chronic respiratory disease, and the reasons are layered:
Air quality crisis: India is home to many of the world’s most polluted cities. PM2.5 concentrations in Delhi, Patna, and several other major cities regularly exceed WHO guidelines by 10–20 times. Chronic exposure to PM2.5 is directly linked to COPD development, asthma worsening, and increased acute bronchitis episodes.
Indoor air pollution: Despite urban awareness, approximately 60% of Indian households still rely on solid biomass fuels for cooking, exposing household members — predominantly women and children — to smoke equivalent to smoking several packs of cigarettes daily. This is a leading cause of COPD in non-smoking Indian women, a pattern very different from Western countries.
The tobacco burden: India has approximately 267 million tobacco users. Bidis (small leaf-wrapped cigarettes) are prevalent and arguably more harmful per cigarette than manufactured cigarettes due to higher particulate output.
Underdiagnosis epidemic: Studies suggest that over 90% of COPD cases in India go undiagnosed. Spirometry is not routinely available at primary care level, and patients often attribute worsening breathlessness to age, weight, or deconditioning — seeking care only when severely compromised.
Asthma mismanagement: Many asthma patients in India are prescribed oral bronchodilators and antibiotics repeatedly for “chest infections” rather than receiving proper inhaler therapy — often due to cost barriers, inhaler stigma, or inadequate primary care.
The convergence of air pollution, tobacco use, biomass fuel exposure, and underdiagnosis creates a respiratory disease burden that demands urgent, specialist-level attention.
When to See a Pulmonologist — and Not to Wait
General practitioners can manage mild cases, but several situations specifically warrant a pulmonologist (respiratory specialist):
- Diagnosis is uncertain: When symptoms don’t clearly fit one condition
- Symptoms are not improving with initial treatment
- Frequent exacerbations: More than 2 respiratory infections or flare-ups per year requiring steroids or antibiotics
- Worsening despite treatment: Progressive breathlessness or declining exercise tolerance
- Severe or difficult-to-control asthma
- Suspected COPD in a smoker or ex-smoker, especially over age 40
- Before starting biologic therapy for asthma
- Occupational exposure: If symptoms may be work-related
- Child with recurrent wheeze: To confirm whether it’s asthma and initiate appropriate preventive therapy
Don’t normalize breathlessness. Many patients — particularly those with COPD — gradually reduce their activity levels to avoid triggering breathlessness, masking the progression of the disease. By the time they seek care, significant, irreversible lung damage has often occurred.
FAQs: Questions Patients Actually Ask
Q1: Can asthma turn into COPD?
Asthma and COPD are distinct diseases. Asthma itself doesn’t “turn into” COPD. However, poorly controlled asthma over many years causes structural changes (airway remodelling) that can lead to fixed, partially irreversible obstruction — blurring the line between the two. A person with asthma who also smokes significantly accelerates this risk. The term “Asthma-COPD Overlap” (ACO) is used when both conditions coexist.
Q2: Is bronchitis contagious?
Acute bronchitis caused by a viral infection is contagious — the same way a cold or flu is. Transmission is through respiratory droplets and hand-to-surface contact. Chronic bronchitis, however, is not contagious — it’s a structural, inflammatory condition driven by long-term irritant exposure, not an active infection that can spread.
Q3: Can COPD be cured?
Currently, no. COPD involves permanent destruction of lung tissue and structural airway changes that cannot be reversed. However, progression can be significantly slowed — especially with smoking cessation — and quality of life can be dramatically improved with modern treatments, pulmonary rehabilitation, and proper management of exacerbations. “Can’t be cured” does not mean “nothing can be done.”
Q4: I have asthma but I also smoke. Am I definitely going to get COPD?
Smoking with asthma creates a compounded risk. Tobacco smoke is both a potent asthma trigger and the leading cause of COPD. People who smoke with asthma are much more likely to develop ACO (Asthma-COPD Overlap) and to experience accelerated lung function decline. Quitting smoking is the highest-impact action an asthmatic smoker can take.
Q5: My X-ray came back normal. Does that mean I don’t have asthma or COPD?
A normal chest X-ray does not rule out asthma or early-to-moderate COPD. Both conditions are diagnosed primarily through spirometry (lung function testing), not imaging. X-rays are useful to rule out other conditions (pneumonia, lung mass) or confirm changes in severe COPD, but normal imaging is common in well-controlled asthma and early COPD.
Q6: Can children get COPD?
Classic COPD in the adult sense is rare in children. However, children with severe or recurrent respiratory infections, or those with certain genetic conditions (like Alpha-1 antitrypsin deficiency), can develop COPD-like changes in lung structure early in life. Severe childhood lung disease is also increasingly recognized as a risk factor for COPD in adulthood.
Q7: My doctor prescribed inhalers for bronchitis. Is that right?
It depends. If you have bronchitis with underlying asthma, a bronchodilator inhaler is appropriate. For otherwise-healthy individuals with simple acute bronchitis (no asthma), inhalers don’t provide additional benefit beyond what the body will do naturally. Your doctor may prescribe an inhaler if they suspect there’s an asthmatic component, if you’re wheezing, or to facilitate faster symptom resolution — but it’s worth asking for clarification.
Conclusion: Precision Matters When You Can’t Breathe
Asthma, COPD, and bronchitis may share the surface symptoms of coughing and breathlessness — but underneath, they are fundamentally different diseases with different causes, different trajectories, and different treatments.
Asthma is a reversible, inflammatory disease of the airways that can be excellently controlled with the right therapy. COPD is a slow-burning, progressive disease where early diagnosis and lifestyle change — above all, stopping smoking — can preserve years of healthy life. Bronchitis is either a self-resolving acute illness or a chronic warning sign that something more serious is affecting your lungs.
The pattern in India — rising pollution, widespread biomass fuel use, high tobacco consumption, and a chronic shortage of accessible spirometry — makes accurate respiratory diagnosis not just a clinical matter but a public health imperative.
Breathing is not something to compromise on. If you’ve been managing recurring symptoms with generic cough syrups and antibiotic courses without a clear diagnosis, it’s time for a proper lung function evaluation.

