
Your lungs have more untapped capacity than you think. Here’s how to access it.
Most people use only about 50–60% of their lung capacity during ordinary breathing. That’s not a flaw — it’s physiological reserve, the buffer your body keeps in storage for moments of demand. But for the millions of people managing asthma, COPD, post-COVID breathlessness, or simply the cumulative effect of years spent breathing polluted urban air, that reserve shrinks. And unlike muscle mass or cardiovascular fitness, most people never think to train it back.
Breathing exercises — what pulmonologists call respiratory muscle training or ventilatory training — are one of the few evidence-backed interventions that can genuinely improve the mechanical efficiency of your lungs, strengthen the muscles that drive breathing, and meaningfully reduce breathlessness in everyday life. They cost nothing, carry virtually no risk when done correctly, and require no equipment.
This guide covers seven doctor-recommended techniques with step-by-step instructions and the clinical rationale behind each — not just what to do, but why it works, who it helps most, and what to be careful about.
First, What Does “Lung Capacity” Actually Mean?
Lung capacity is not a single number — it’s a family of related measurements that together describe how your lungs function. Understanding the relevant terms helps explain why different exercises target different problems.
Tidal volume is the amount of air you move in and out during a normal, effortless breath — roughly 500ml in a healthy adult. This is the air you exchange at rest without conscious effort.
Vital capacity (VC) is the maximum amount of air you can exhale after taking the deepest possible breath. In a healthy adult, this is roughly 3.5–5 litres depending on age, sex, and height. Vital capacity is reduced in both obstructive conditions (asthma, COPD) and restrictive conditions (pulmonary fibrosis).
Total lung capacity (TLC) is the maximum volume of air the lungs can hold — including the residual volume that always stays in your lungs to prevent them from collapsing. For a healthy adult, this is approximately 6 litres.
Functional residual capacity (FRC) is the air remaining in the lungs after a normal, passive exhalation — your “resting volume.” In COPD and emphysema, air trapping causes FRC to increase, making each subsequent breath feel like it’s starting from a fuller, less comfortable position. This is the physiological basis for the characteristic breathlessness of COPD.
FEV1 (Forced Expiratory Volume in 1 second) is the volume of air expelled in the first second of a forceful exhalation — the primary spirometry measurement used to diagnose and grade obstructive lung disease.
Most breathing exercises don’t directly increase total lung capacity (TLC is largely determined by lung size, which is fixed by adulthood). What they do — and this is clinically significant — is improve the efficiency with which you use existing capacity, strengthen the respiratory muscles that drive airflow, reduce dynamic hyperinflation (air trapping) in COPD, and lower the perceived effort of breathing. For people with chronic respiratory disease, this can make a larger practical difference than the raw numbers suggest.
The Respiratory Muscles: What You’re Actually Training
Most people think of breathing as a passive process. It isn’t. Breathing is driven by a sophisticated coordinated contraction of several muscle groups.
The diaphragm is the primary muscle of breathing — a dome-shaped sheet of muscle that sits beneath the lungs and separates the thoracic and abdominal cavities. When it contracts, it flattens downward, expanding the thoracic cavity and creating negative pressure that draws air in. At rest, the diaphragm should do approximately 70–80% of the work of breathing in a healthy person.
Intercostal muscles (between the ribs) expand and lift the rib cage during inhalation, supplementing the diaphragm.
Accessory muscles — the sternocleidomastoid and scalene muscles in the neck, and the pectorals and serratus muscles in the chest — are recruited during exercise or respiratory distress when additional inspiratory force is needed.
In many people with chronic respiratory disease — and even in healthy people who habitually breathe shallowly — the diaphragm becomes underused and the accessory muscles take over. This is inefficient: accessory muscle breathing is energetically costly, produces less airflow per unit of effort, and contributes to the sensation of breathlessness and fatigue. Diaphragmatic breathing exercises specifically address this pattern.
7 Doctor-Recommended Breathing Exercises
1. Diaphragmatic Breathing (Belly Breathing)

Diaphragmatic breathing is the foundation of respiratory muscle training and the technique most consistently recommended by pulmonologists and respiratory physiotherapists. If you only learn one exercise from this guide, make it this one.
Why it works: In people who habitually breathe with their chest (accessory-muscle-dominant breathing), the diaphragm is underutilised. Consciously re-engaging it during practice gradually restores it to its primary role, making each breath more mechanically efficient. Studies in COPD patients have shown diaphragmatic breathing reduces respiratory rate, increases tidal volume, and improves arterial oxygen saturation during practice. In healthy individuals, it significantly reduces breathing effort and can lower anxiety-driven hyperventilation.
How to practise:
- Lie on your back with knees slightly bent, or sit in a supported chair. Wearing loose clothing makes abdominal movement easier to observe.
- Place one hand flat on your chest and one on your abdomen, just below the ribcage.
- Inhale slowly and deeply through your nose over 3–4 seconds. The goal is for your abdominal hand to rise while your chest hand remains relatively still. If your chest is rising first or prominently, you’re recruiting chest muscles rather than your diaphragm.
- At the top of the breath, pause briefly without forcing.
- Exhale slowly through your mouth or nose over 4–6 seconds. Feel your abdominal hand fall as the diaphragm releases back upward.
- Aim for 6–8 breaths per minute rather than your normal unconscious rate of 12–20.
Practice: 5–10 minutes, twice daily. Progress to practising in seated, standing, and eventually moving positions as the pattern becomes more automatic.
Best for: Everyone as a foundation technique; especially COPD, anxiety-related breathlessness, post-surgical recovery, and anyone retraining breathing mechanics after a period of illness.
2. Pursed-Lip Breathing
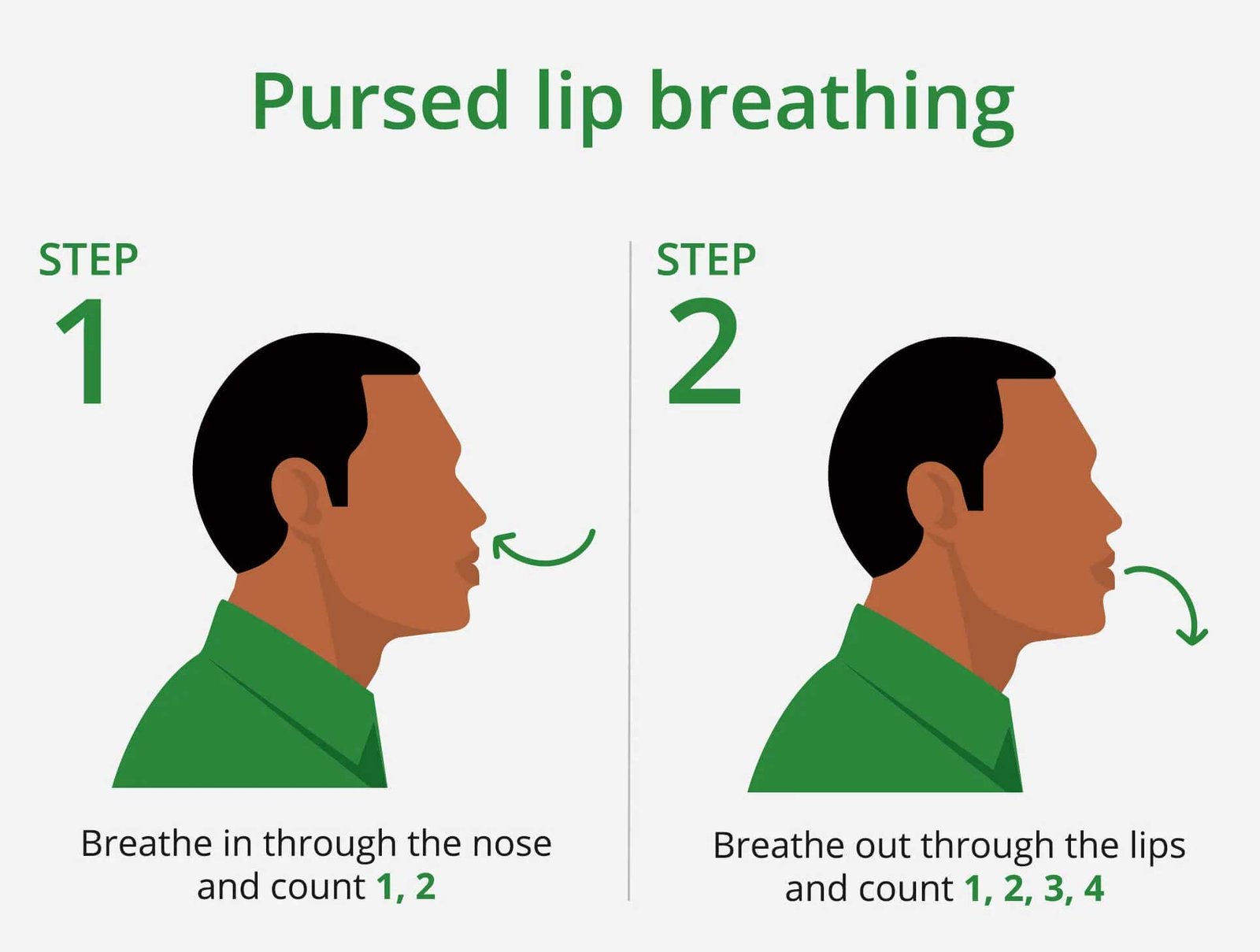
Pursed-lip breathing is one of the most clinically studied breathing techniques and has strong evidence behind it, particularly for COPD.
Why it works: When you exhale through pursed lips — creating a slight resistance at the mouth — you generate a small amount of back-pressure in the airways. This pressure is transmitted back into the bronchioles, helping to keep them open throughout exhalation. In healthy airways, this isn’t necessary because the airway walls are structurally supported. In COPD, where the airway walls have lost elasticity, they tend to collapse inward during exhalation, trapping air and increasing FRC. Pursed-lip breathing counteracts this collapse, allowing more complete emptying of the lungs with each breath. The result: less air trapping, lower FRC, and more room for the next breath.
How to practise:
- Sit upright or stand — avoid lying down for this exercise.
- Inhale slowly through your nose over 2 seconds. A normal-depth breath is fine; you don’t need a maximal inhalation.
- Pucker your lips as if you’re about to whistle, blow out a candle, or kiss someone — there should be a small, deliberate gap between them.
- Exhale slowly and steadily through the pursed lips over 4 seconds — roughly twice as long as the inhalation. The airflow should be gentle, not forceful. If you can blow out a candle a foot away, you’re exhaling too hard.
- The exhalation should feel slightly effortful but not strained. A faint resistance sensation is normal and intentional.
Practice: Use during any activity that triggers breathlessness — climbing stairs, walking, carrying anything. It’s most useful as a real-time intervention during exertion, not just as a timed exercise.
Best for: COPD (particularly emphysema-dominant), anyone experiencing dynamic air trapping, exercise-induced breathlessness, anxiety-related breathing pattern disorders.
3. Deep Breathing with Breath Hold (Sustained Maximal Inspiration)

This technique — formally called sustained maximal inspiration or incentive spirometry when done with a device — is used in respiratory physiotherapy to recruit alveoli that have collapsed or become underventilated.
Why it works: Parts of the lung — particularly the bases — can gradually become underventilated in people who habitually breathe shallowly, spend long periods in bed, or are recovering from illness or surgery. Alveoli that are chronically underinflated can undergo microatelectasis (small-scale collapse). Deep, sustained inspiration reinflates these regions, restores ventilation to underused lung zones, and activates the collateral ventilation channels (pores of Kohn) that allow air to pass between alveoli via alternative pathways.
How to practise:
- Sit upright, which allows the diaphragm to descend further than in a lying position.
- Begin with a normal exhalation to clear the lungs.
- Inhale as slowly and deeply as possible through your nose, aiming for a 5–6 second inhalation. Focus on expanding your rib cage laterally (sideways) and the lower chest, not just the upper chest.
- At the top of the breath, hold gently for 3–5 seconds. This hold allows air to redistribute to slower-filling lung regions.
- Exhale slowly and completely over 5–6 seconds.
- Take 2–3 normal breaths before repeating.
Practice: 5–10 repetitions per session, 2–3 times daily. More than this can cause dizziness from altered blood CO2 levels.
Best for: Post-operative recovery, bedridden patients preventing pneumonia, post-COVID recovery with residual breathlessness, anyone with a restrictive ventilatory pattern.
4. Alternate Nostril Breathing (Anulom Vilom / Nadi Shodhana)

Anulom Vilom — the classical yoga pranayama practice — has moved from traditional practice into the respiratory research literature over the past two decades, with a growing body of evidence supporting its effects on lung function, cardiovascular autonomic balance, and stress physiology.
Why it works: Each nostril has preferential airflow that alternates roughly every 90–120 minutes in healthy people — a phenomenon called the nasal cycle, regulated by the autonomic nervous system. The right nostril is associated with sympathetic activation; the left with parasympathetic. Alternately breathing through each nostril may modulate this autonomic balance. From a purely mechanical standpoint, the resistance created by breathing through a single nostril increases the duration and effort of inhalation, providing mild resistive training to respiratory muscles. A 2017 study in the Indian Journal of Physiology and Pharmacology found that 12 weeks of alternate nostril breathing practice significantly improved FVC, FEV1, and peak expiratory flow in healthy adults.
How to practise:
- Sit comfortably with your spine upright. Rest your left hand on your knee.
- Bring your right hand to your face: fold the index and middle fingers toward the palm, leaving the thumb, ring finger, and little finger extended. The thumb will close the right nostril; the ring finger will close the left.
- Close the right nostril with your thumb. Inhale slowly and completely through the left nostril over 4 seconds.
- Close both nostrils briefly at the top of the breath (1–2 seconds).
- Release the right nostril and exhale completely through the right nostril over 4–8 seconds.
- Inhale through the right nostril (left still closed) over 4 seconds.
- Close both nostrils at the top.
- Release the left nostril and exhale through the left over 4–8 seconds.
- This completes one full cycle. Aim for 5–10 cycles.
Practice: 5–10 minutes daily, ideally in the morning before eating.
Best for: General lung health maintenance, stress-related breathing pattern disorders, hypertension with respiratory component, athletes seeking performance optimization, anyone finding Western breathing exercises too clinical.
5. Box Breathing (Four-Square Breathing)
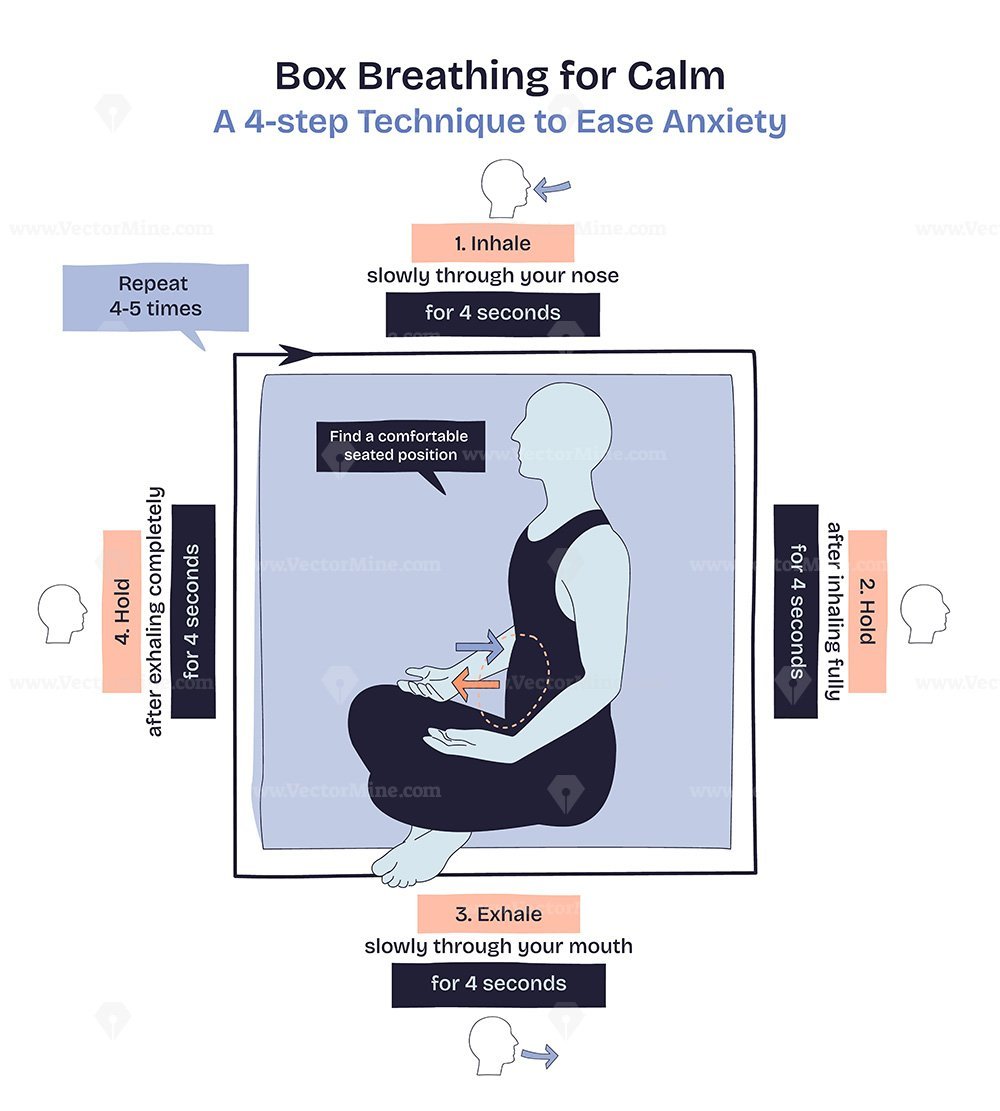
Box breathing — four equal phases of inhale, hold, exhale, hold — was developed in military and elite performance contexts but has solid physiological grounding and is increasingly used in respiratory rehabilitation.
Why it works: The prolonged, deliberate breath cycle overrides the automatic breathing pattern driven by brainstem respiratory centres, temporarily bringing the breath under voluntary cortical control. This has two effects: it significantly activates the parasympathetic nervous system (reducing heart rate, cortisol, and the perception of breathlessness), and it trains the respiratory muscles through the sustained holds. The exhalation hold, specifically, creates a period of controlled hypoxic stimulus that research suggests may improve peripheral oxygen utilisation over time. For people with anxiety-linked respiratory symptoms — a very common pattern — the predictable, counting-based structure of box breathing provides an effective cognitive anchor.
How to practise:
- Sit upright or lie flat. Close your eyes.
- Exhale completely to clear the lungs before beginning.
- Inhale slowly through your nose over exactly 4 seconds.
- Hold the breath at the top — lungs full — for 4 seconds. Maintain a gentle, comfortable hold rather than a strain.
- Exhale through your nose or mouth over 4 seconds.
- Hold at the bottom — lungs empty — for 4 seconds before the next inhale.
- This is one box. Aim for 4–6 boxes per session.
As the technique becomes comfortable, you can extend to a 5-5-5-5 or 6-6-6-6 pattern.
Practice: Use proactively (before a stressful situation or exercise) or reactively (during a breathlessness episode to regain control of breathing pattern).
Best for: Anxiety-driven hyperventilation, stress-related breathing pattern disorders, performance contexts (sports, public speaking), general stress management with respiratory benefit.
6. Lateral Costal (Rib Expansion) Breathing

This technique specifically targets lateral expansion of the thoracic cage — the sideways rib movement that is often neglected in habitual shallow breathing.
Why it works: The lower lobes of the lungs extend laterally and posteriorly, not just downward. Most people’s habitual breathing pattern recruits the upper chest preferentially, leaving the lateral and posterior lung bases chronically underventilated. Lateral costal breathing directs airflow into these underused regions, improving the distribution of ventilation across the lung. It also directly trains the external intercostal muscles, improving rib cage mobility — something that reduces in COPD and other chronic respiratory conditions over time.
How to practise:
- Stand upright or sit with your spine straight.
- Place your hands on the sides of your rib cage — not on the front of your chest, but the lateral surfaces, roughly below the armpits.
- Take a deep breath in, consciously directing the air to push your hands outward and sideways. The goal is lateral rib cage expansion, not upward shoulder movement.
- At the top of the breath, hold for 3–5 seconds and consciously feel the outward pressure against your hands.
- Exhale slowly and completely, feeling the ribs return inward.
- Repeat 5–8 times.
Practice: 5 minutes once or twice daily. Particularly effective before exercise.
Best for: Post-operative recovery (especially abdominal or thoracic surgery), COPD with restricted rib cage mobility, people with desk-bound postures who have developed forward-flexed thoracic posture, pre- and post-natal respiratory training.
7. Humming Exhalation (Bhramari Pranayama)

The humming breath — known in yoga as Bhramari (bee breath) — produces vibration throughout the airways and sinuses during exhalation and has a surprisingly interesting physiological mechanism.
Why it works: Humming during exhalation dramatically increases nasal nitric oxide (NO) production — research published in the American Journal of Respiratory and Critical Care Medicine found that humming increased nasal NO concentrations by a factor of 15 compared to silent exhalation. Nitric oxide is a potent bronchodilator and vasodilator; it relaxes airway smooth muscle and improves mucociliary clearance (the mechanism by which the airways clear mucus and particles). Beyond the NO effect, the audible vibration created by humming provides a form of airway oscillation comparable to some commercial airway clearance devices (like flutter valves), helping to mobilise secretions. The technique also significantly prolongs exhalation, producing parasympathetic activation similar to other slow-breathing techniques.
How to practise:
- Sit comfortably with eyes closed.
- Inhale deeply through the nose over 4–5 seconds.
- As you exhale, produce a steady, consistent humming sound — the pitch doesn’t matter. The hum should be gentle and continuous, not strained. You should feel vibration in your nose, face, and chest.
- Continue the hum for the entire exhalation — typically 6–10 seconds.
- Take one normal breath, then repeat.
- Aim for 8–10 repetitions.
Practice: 5–8 minutes daily, ideally in a quiet setting. Can be used during acute congestion to help clear secretions.
Best for: Chronic sinusitis, bronchiectasis (where airway secretion clearance is impaired), asthma with mucus hypersecretion, anxiety and stress, anyone who responds well to sound-based practices.
How Often Should You Practise?
There is no universal prescription, but the research and clinical practice guidelines converge on a few principles:
Frequency matters more than duration. Daily practice for 10–15 minutes produces better results than an occasional 45-minute session. The goal is to gradually retrain automatic breathing patterns — which requires consistent repetition.
Twice daily is the evidence-supported standard for people practising as part of rehabilitation (COPD, post-COVID, post-surgical). For healthy individuals practising for maintenance and performance, once daily is adequate.
Build progressively. Start with one or two techniques until they feel natural, then layer in others. Attempting all seven at once leads to cognitive overload and poor technique execution.
The best time of day is the time you’ll actually do it. Morning practice before meals is physiologically ideal (airways are most reactive in the early morning, which is when these techniques provide the most benefit for asthma and COPD). But consistency trumps timing — a noon or evening session every day beats a morning session twice a week.
Who Benefits Most — and Who Should Be Careful
These exercises are well-suited for:
People with stable asthma — particularly diaphragmatic breathing and pursed-lip breathing, which improve breathing efficiency and can reduce rescue inhaler use by addressing panic-breathing patterns that worsen attacks.
COPD patients — pursed-lip breathing and diaphragmatic breathing have the strongest evidence base here. A Cochrane review of breathing exercises in COPD found significant improvements in dyspnoea (breathlessness) scores, exercise capacity, and quality of life.
Post-COVID recovery — the phenomenon of persistent breathlessness after COVID-19 is complex and not fully understood, but respiratory muscle weakness, deconditioning, and breathing pattern disorder (dysfunctional breathing) are significant contributors. Diaphragmatic breathing, deep breathing, and lateral costal breathing specifically address these mechanisms.
Athletes seeking performance improvement — inspiratory muscle training (a formalised version of resistive breathing exercises) is well-studied in sports science, with evidence of improved endurance performance in competitive athletes.
Healthy adults in high-pollution environments — regular breathing exercises improve mucociliary clearance and respiratory muscle efficiency, providing some resilience against the effects of chronic pollutant exposure.
People with anxiety — breathing pattern disorder (dysfunctional breathing driven by anxiety) is far more common than typically recognised. Box breathing and diaphragmatic breathing are first-line interventions.
Use caution or consult your pulmonologist first if:
You have severe COPD (GOLD Stage 3–4), where diaphragmatic breathing in particular can paradoxically worsen breathlessness in some patients due to the altered geometry of an overinflated thorax. A physiotherapist should supervise initial practice.
You are in an acute exacerbation of any respiratory condition — breathing exercises are for stable states, not acute crises. During an active asthma attack or COPD flare, focus on pursuing-lip breathing as a symptom management tool, and seek medical care.
You have recent rib fractures, pneumothorax history, or recent thoracic surgery — consult your surgeon or respiratory physiotherapist before starting.
You experience dizziness, tingling, or faintness during practice — this is most commonly caused by hypocapnia (low CO2 from overbeathing) and means you’re breathing too deeply or too rapidly. Slow down, reduce the depth of inhalation, and let normal breathing resume.
Breathing Exercises and Post-COVID Recovery: A Closer Look
Long COVID — the persistence of symptoms beyond four weeks after acute infection — affects an estimated 10–30% of COVID-19 survivors. Breathlessness is one of the most common and disabling post-COVID symptoms, often persisting months after the acute illness has resolved.
The mechanisms of post-COVID breathlessness are heterogeneous:
- Residual pulmonary inflammation in some patients with severe initial infection
- Deconditioning — particularly relevant in those who were significantly ill or hospitalised
- Breathing pattern disorder — arguably the most underdiagnosed contributor: dysregulation of the automatic breathing pattern driven by the neurological and autonomic effects of COVID-19
- Respiratory muscle weakness from prolonged illness, reduced activity, and in some cases from the direct effects of the virus on muscle tissue
- Anxiety and hyperventilation — a common and self-reinforcing cycle
Breathing exercises — particularly diaphragmatic breathing, deep breathing, and lateral costal breathing — directly address the last three mechanisms. They do not reverse pulmonary fibrosis or inflammation, but for the large proportion of post-COVID patients whose breathlessness is driven by pattern disorder and deconditioning rather than fixed lung damage, they can produce dramatic improvements.
A structured respiratory physiotherapy programme — which can be conducted via teleconsultation with appropriate guidance — is one of the most evidence-supported interventions for this population and is recommended by NICE (National Institute for Health and Care Excellence) guidelines for post-COVID management.
The India Context: Why Breathing Exercises Are Not Optional

For people living in Indian cities, respiratory muscle training is not a wellness luxury — it is a practical, compensatory health measure.
The average PM2.5 concentration in Delhi for the winter months consistently exceeds 150–200 μg/m³ — compared to the WHO safe limit of 5 μg/m³ annually and 15 μg/m³ for 24-hour exposure. Breathing this air chronically causes airway inflammation, accelerates lung function decline, and increases susceptibility to respiratory infection. For someone already managing asthma or COPD, these concentrations can trigger acute exacerbations within hours of exposure.
What breathing exercises can and cannot do in this context: they cannot neutralise the effects of pollutant inhalation. They can meaningfully improve mucociliary clearance (the airway’s defence mechanism for clearing inhaled particles), strengthen the respiratory muscles to reduce the impact of increased breathing effort during high-pollution days, and reduce the anxiety-driven hyperventilation that pollution-related breathlessness often triggers.
They should be part of a broader strategy that includes N95 mask use during high-pollution periods, indoor HEPA filtration, minimising outdoor exercise during peak pollution hours (early morning and evening in winter months), and regular respiratory monitoring for those with existing lung disease.
Complementary Lifestyle Measures
Breathing exercises work best as part of a broader approach to respiratory health.
Aerobic exercise is the most powerful single intervention for improving cardiovascular and respiratory fitness. It increases the efficiency of oxygen extraction at the tissue level, reducing the demand on the lungs for any given level of activity. Even 20–30 minutes of brisk walking five days per week produces measurable improvements in FEV1 and exercise tolerance in people with mild-to-moderate COPD.
Posture has a direct mechanical effect on breathing. A forward-flexed, rounded-shoulder posture — extremely common in desk-working populations — compresses the thoracic cage and limits diaphragmatic descent. Even modest improvements in thoracic extension and shoulder position measurably increase breathing capacity.
Hydration maintains the appropriate viscosity of airway secretions. Dehydration makes secretions thicker and harder to clear, increasing the risk of infection and worsening chronic cough.
Smoking cessation should precede, accompany, and never be replaced by breathing exercises. No exercise programme can compensate for the ongoing airway damage caused by active smoking.
Singing and wind instrument playing — genuinely evidence-supported for respiratory muscle training, particularly in older adults and COPD patients. The sustained, controlled exhalation required for singing provides inspiratory muscle load and prolongs expiratory time in a way that closely mirrors therapeutic breathing exercises.
FAQs
Q1: Can breathing exercises actually increase lung capacity? Technically, total lung capacity (the maximum volume the lungs can hold) is determined by lung size, which is largely fixed in adulthood. What breathing exercises reliably improve is functional capacity — the efficiency with which you use existing lung volume, the strength and endurance of respiratory muscles, and the reduction of air trapping in obstructive disease. For most people, this functional improvement is more meaningful in daily life than the raw TLC number.
Q2: How long before I notice any difference? Most people report reduced breathlessness during daily activities within 2–4 weeks of consistent daily practice. Measurable improvements in spirometry (FEV1, FVC) typically appear after 6–8 weeks of regular practice in people with obstructive disease. Subjective wellbeing improvements — including sleep quality, energy levels, and reduced anxiety — often appear within the first week.
Q3: Can I do these exercises during an asthma attack? During an acute attack, your priority is rescue inhaler use and seeking emergency care if the attack is severe. Pursed-lip breathing can help maintain some degree of airway patency during mild breathlessness and can prevent panic-breathing that worsens attacks. However, attempting to practise new breathing techniques during a significant attack is not appropriate. The value of these exercises is in reducing the frequency and severity of attacks through regular training — not in managing the acute event itself.
Q4: Are these exercises safe during pregnancy? With the exception of extended breath holds (which should be avoided in pregnancy), all the exercises described here are safe and beneficial during pregnancy. Pregnancy progressively reduces lung capacity by compressing the diaphragm, and diaphragmatic and lateral costal breathing are specifically recommended by obstetric physiotherapists to maintain respiratory efficiency as the uterus expands.
Q5: Can children do these exercises? Yes, from approximately age 6–7 when they can understand and follow instructions. Diaphragmatic breathing and pursed-lip breathing in particular are recommended for children with asthma as part of non-pharmacological management. Box breathing is an effective anxiety-management tool for older children and adolescents.
Conclusion: The Simplest Form of Lung Training
Your respiratory muscles — like all muscles — respond to training. Unlike most other forms of exercise, breathing training requires no equipment, minimal time, and no physical exertion. It can be done sitting in an office chair, lying in a hospital bed, or standing in a queue.
The science is clear: consistent practice of the techniques described here produces measurable, clinically meaningful improvements in breathing efficiency, exercise tolerance, and quality of life — particularly for people managing chronic respiratory disease, recovering from COVID-19, or living in high-pollution environments.
Start with diaphragmatic breathing. Master it until it feels natural. Then layer in pursed-lip breathing if you have COPD or air trapping. Add the technique that appeals most to you personally — because the best breathing exercise is the one you’ll actually practise every day.
